
Below you will find data related to posters that will be presented at the 2026 FNDS meeting.
See their website here
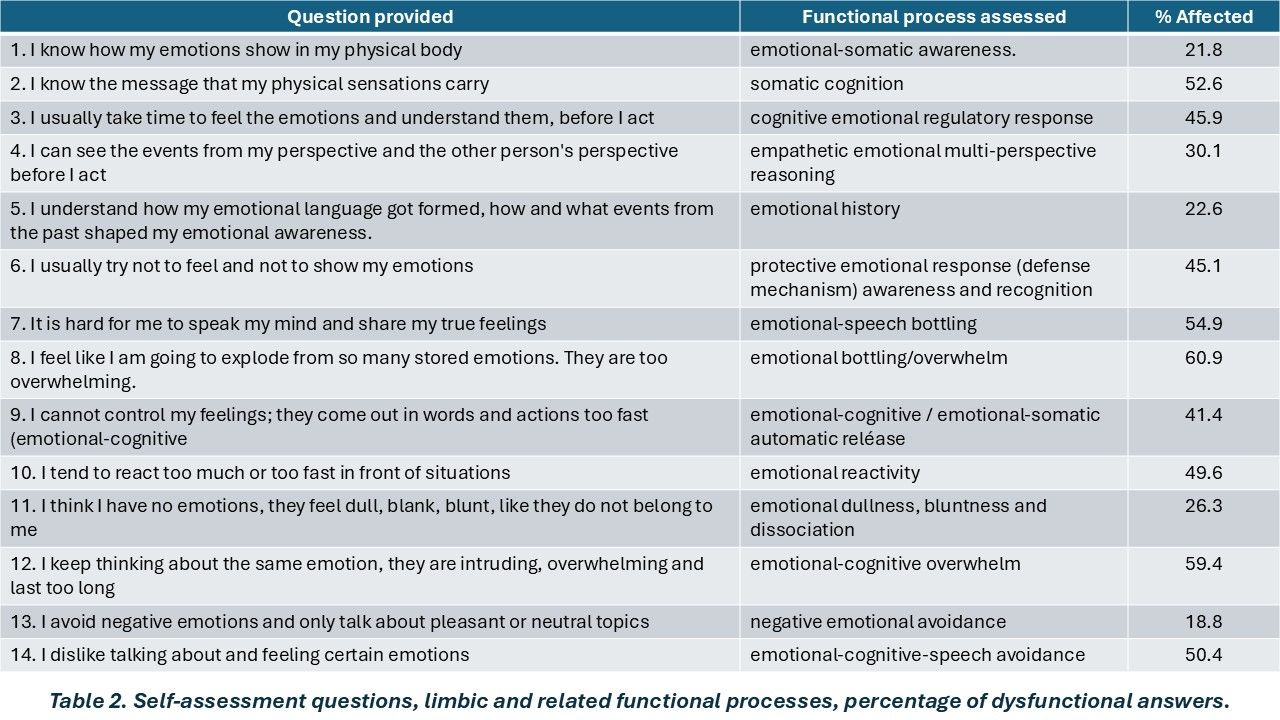
Poster #1. Assessment of 14 limbic and interrelated networks’ functional processes in 133 individuals.
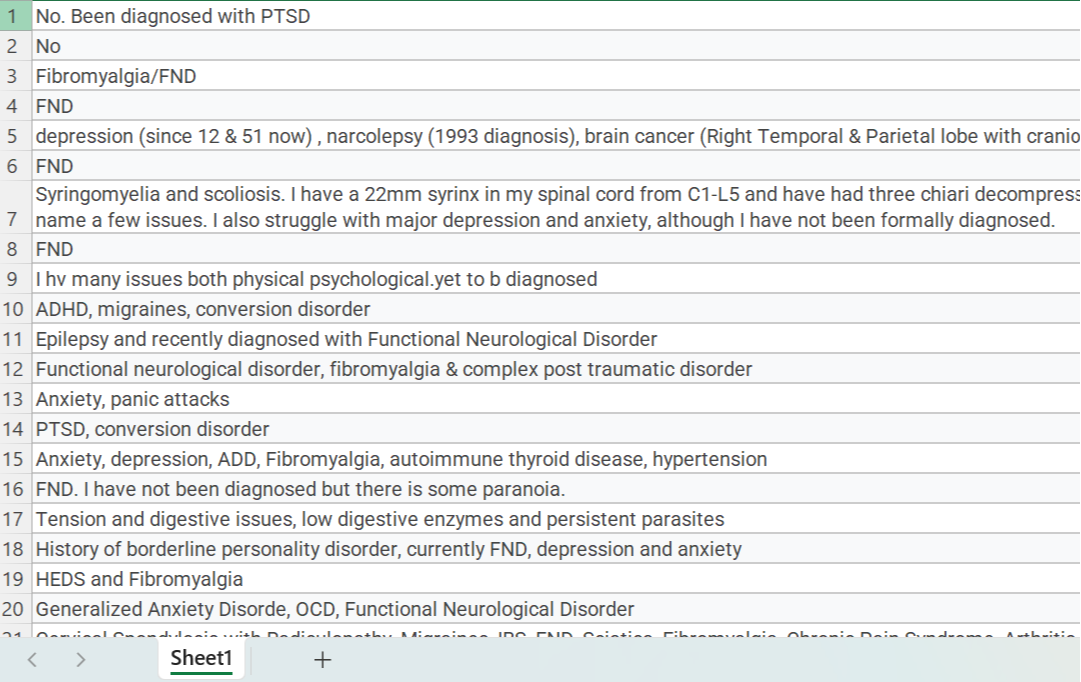
Table 1. Functional and physical medical conditions reported by respondents.
(Touch on the image to download Excel file).
----------------------------------------------------------------
Poster #2. Subjective Functional Markers after 2 years of
EXPERIENTIAL EDUCATION METHODOLOGY.
Level 3 assessment. Participants 1-5





Level 4 assessment. Participants 1-5





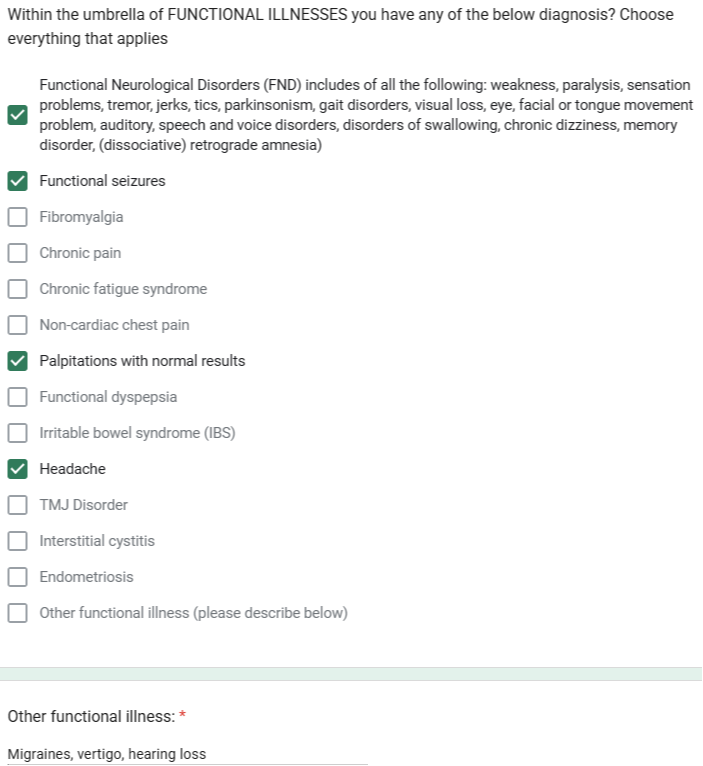
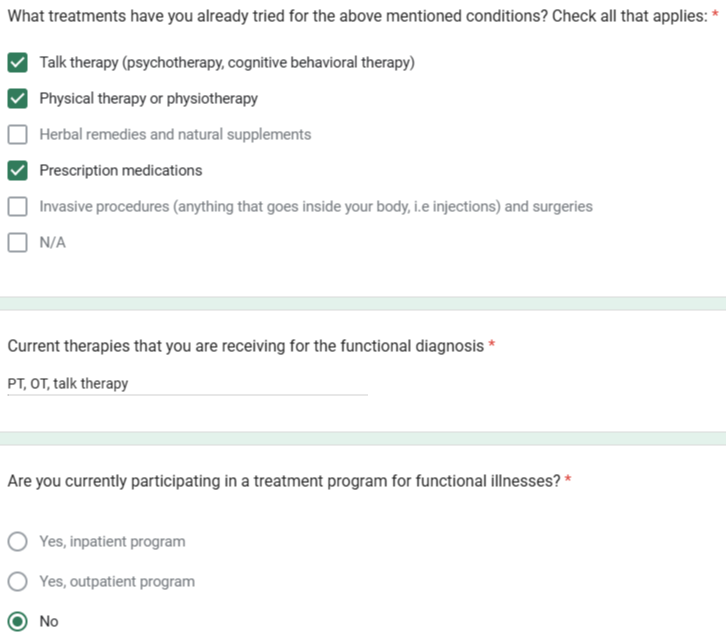
Download Database 1 (participants’ demographics, diagnosis, previous treatments used and other characteristics of interest in excel form) BY CLICKING IN THE BELOW IMAGE
-----------------------------------------------------------------------------
Join Our Newsletter
(sent monthly to every 3 months)
